
Feeling a little lost as you start to compile your first 510(k) submission?
You’re not alone.
There is all this information out there to try and help you, but it can be overwhelming trying to sift through. As you likely already know, the majority of 510(k) submissions are rejected the first time. Maybe you’ve already had yours kicked back to you once or twice.
This step-by-step guide to preparing your 510(k) submission aims to put the requirements in easy-to-understand terms and includes some helpful, actionable and practical tips you can begin to implement immediately. The goal of this guide is to provide you step-by-step guidance through each part of the FDA 510(k) submission process and help improve your time to market.
To start, here’s a list of all the sections required in a 510(k) submission:
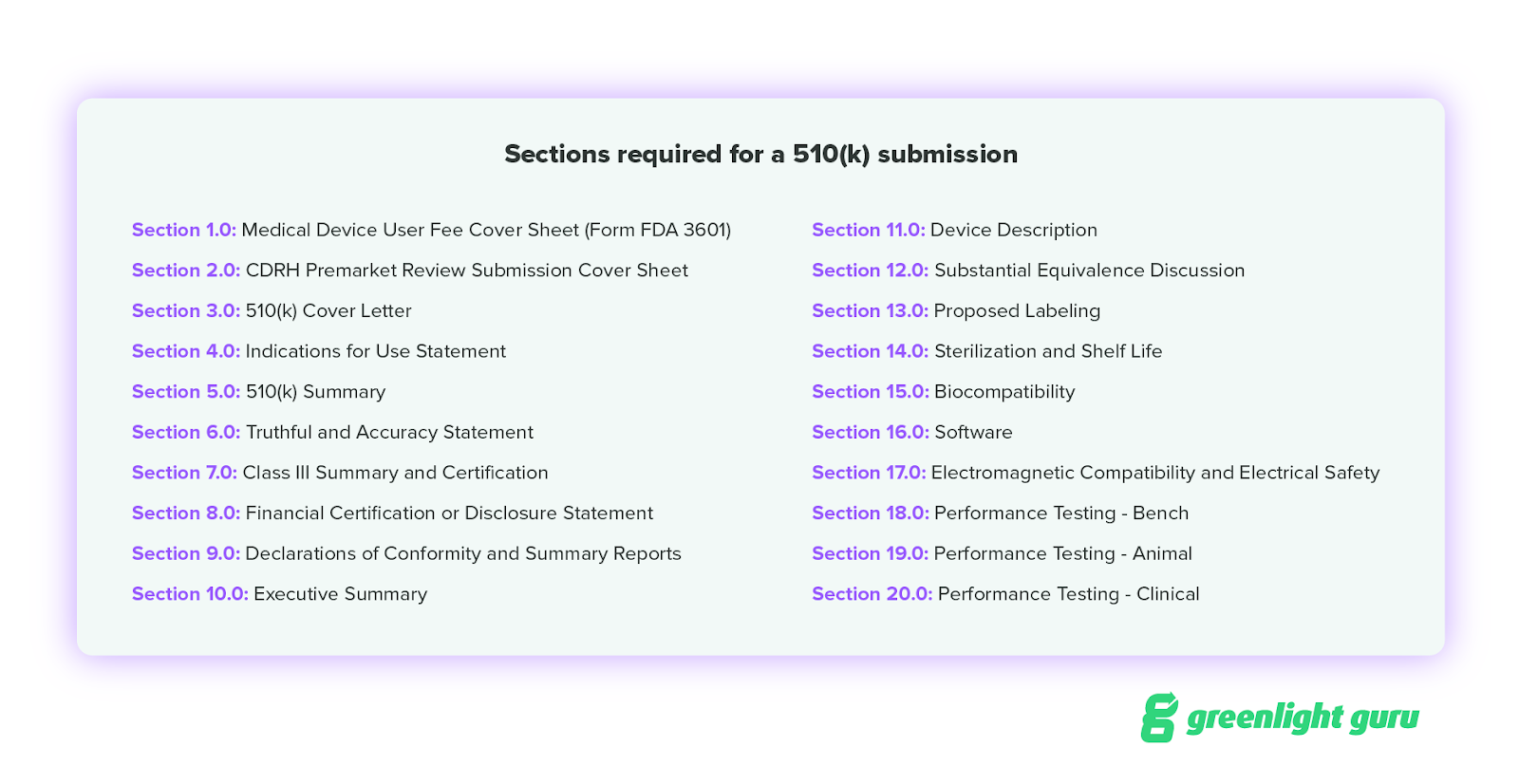
Throughout the guide you’ll notice we’ve grouped certain sections of the 510(k) submission together. These sections are typically related and tend to be focused on similar topics. It’s also easier to bite off smaller chunks than to try and tackle it all at once.
You can jump to any of these groups by clicking on the links below:
Group 1 – Cover Sheet Forms
Section 1.0 – Medical Device User Fee Cover Sheet (Form FDA 3601)
Section 2.0 – CDRH Premarket Review Submission Cover Sheet
Group 2 – Public Information About Your Device
Section 3.0 – 510(k) Cover Letter
Section 4.0 – Indications for Use Statement
Section 5.0 – 510(k) Summary
Group 3 – Templated Sections
Section 6.0 – Truthful and Accuracy Statement
Section 7.0 – Class III Summary and Certification
Section 8.0 – Financial Certification or Disclosure Statement
Section 9.0 – Declarations of Conformity and Summary Reports
Group 4 – Comparing Your Device vs. Predicate(s)
Section 10.0 – Executive Summary
Section 11.0 – Device Description
Section 12.0 – Substantial Equivalence Discussion
Group 5 – Ensuring Patient Safety
Section 13.0 – Proposed Labeling
Section 14.0 – Sterilization and Shelf Life
Section 15.0 – Biocompatibility
Group 6 – Software and Electrically Powered Components
Section 16.0 – Software
Section 17.0 – Electromagnetic Compatibility and Electrical Safety
Group 7 – Performance Testing
Section 18.0 Performance Testing – Bench
Section 19.0 Performance Testing – Animal
Section 20.0 Performance Testing – Clinical
Before you start: timeline and preparation
If your device will go through the 510(k) pathway, you should be building your submission documentation from day one of product development. Not because the FDA requires it at that stage, but because the sections that take the most time (device description, substantial equivalence discussion, performance testing, biocompatibility) are all pulling directly from your design outputs, your design verification and validation records, and your risk management file. If those records are complete and organized, compiling Groups 4 through 7 of your submission is mostly organization. If they're not, you're doing cleanup and reconstruction under pressure, and that is where timelines slip by months.
Once FDA accepts your submission, the standard review clock is 90 days. In practice, the actual average is longer because FDA frequently issues Additional Information (AI) requests that pause the clock, and many submissions require one or more rounds of back-and-forth before a final decision. First submissions with incomplete sections or mismatched indications for use are the most common source of AI requests and Refuse to Accept (RTA) decisions. Getting the structure right before you file is the most effective way to protect your timeline.
A note on QMSR and current terminology
If you're preparing a 510(k) submission now, you're doing so under the Quality Management System Regulation (QMSR), which went into effect Feb. 2, 2026. The QMSR harmonized FDA's previous Quality System Regulation (QSR) with ISO 13485:2016, and while the underlying documentation requirements are substantially the same, the terminology changed.
The design history file (DHF) is now referred to as the Design and Development File. The device master record (DMR) maps to the Medical Device File. The device history record (DHR) is now referred to as your batch records.
Throughout this guide, you'll see references to DHF and design controls. These are the processes and records that feed directly into the back half of your 510(k) submission. The concepts haven't changed, but if you're organizing your internal documentation under QMSR, use the updated terms to avoid confusion during FDA review. For a full breakdown of what changed under QMSR, visit our QMSR Resource Hub.
Group 1: Cover sheet forms
Section 1.0 – Medical Device User Fee Cover Sheet (Form FDA 3601)
Section 2.0 – CDRH Premarket Review Submission Cover Sheet
The first two sections of your 510(k) submission consist entirely of FDA forms. Both are available directly from the FDA, and the same rule applies to both: always verify you're using the current revision before you use it.
Section 1.0: Medical Device User Fee Cover Sheet (Form FDA 3601)
The Medical Device User Fee Cover Sheet (FDA Form 3601) is essentially a receipt of payment. It captures the type of submission and basic applicant information. You can access it through the FDA's electronic submission gateway, and you'll need to register with the FDA to view and complete it. Once completed, include a printed copy as section 1.0 in your submission package.
Section 2.0: CDRH Premarket Review Submission Cover Sheet
The CDRH Premarket Review Submission Cover Sheet (FDA Form 3514), which runs about five pages and contains nine sections. The first few sections, A through D, are straightforward: type of submission, reason for submission, and applicant information.
It can start to get a little more complicated after that. When you get to Sections E and F, take a few moments to read and re-read the form. Section E is asking about the PREDICATE device. Section F is asking about your device. The two sections run together on the form with only a black line separating them and no white space to help orient you. It’s not uncommon for people to put the predicate device name in section F instead of their product name, so read each section carefully before filling them in.
And finally, remember to check that the indications for use statement on the form matches the indications for use statement used in the rest of the submission. This is one of the biggest reasons FDA rejects 510(k) submissions.
.png)
Group 2: Public information about your device
Section 3.0 – 510(k) Cover Letter
Section 4.0 – Indications for Use Statement
Section 5.0 – 510(k) Summary
Section 3.0: 510(k) Cover Letter
The cover letter contains basic administrative information, the basis for the submission, and a table with information on the design and use of the device. It should be kept fairly straightforward and to the point.
Do be sure your cover letter includes all of the following:
- Type of 510(k) submission, Abbreviated or Traditional
- Your device type in plain terms, i.e., by its common name
- 510(k) submitter
- At least one contact person, by name, title, and phone number
- Your preference for continued confidentiality (21 CFR 807.95)
- Your recommended classification regulation
- Class (i.e., whether it is unclassified or a class I, II, or III device)
- Review panel
- FDA product code
- Any FDA document numbers associated with prior formal correspondence with FDA (e.g., IDE, pre-IDE, 510(k), PMA, request for designation (RFD)) related to your device.
Section 4.0: Indications for Use Statement
The Indications for Use Statement is one of the most consequential sections in the submission. The form itself is FDA Form 3881, but the content is entirely yours to write, and it requires real strategic care.
To establish substantial equivalence, the indications for use of your device must be the same as or narrower than those of your predicate device. Teams often try to get more specific with their indications for use, either to sharpen a marketing claim or to limit the scope of required testing. The problem is that increased specificity doesn't automatically reduce testing requirements. More often, it raises new questions about safety and efficacy, requires additional testing to answer them, or prompts FDA to ask you to select a different predicate. Any of those outcomes adds time to market.
The level of specificity needs to match between your device and the predicate device. Write this section carefully and compare it line by line to your predicate's cleared indications before finalizing.
Section 5.0: 510(k) Summary
The 510(k) Summary is a document that the FDA makes publicly available within 30 days of a substantial equivalence determination. That means whatever you write here will be searchable in the 510(k) database.
FDA will make a 510(k) summary of the safety and effectiveness data available to the public within 30 days of the issuance of a determination that the device is substantially equivalent to another device.
The summary covers information from the cover letter, a summary of the substantial equivalence comparison, and a summary of the testing performed. Because it's public, you're walking a careful line: include enough to meet FDA's minimum requirements without disclosing more competitive or technical detail than necessary.
Group 3: Templated sections
Section 6.0 – Truthful and Accuracy Statement
Section 7.0 – Class III Summary and Certification
Section 8.0 – Financial Certification or Disclosure Statement
Section 9.0 – Declarations of Conformity and Summary Reports
These four sections are the most formulaic in the submission. Most of the content is either pre-written by FDA or a direct response to a binary condition. But a critical rule applies to all of them: if a section doesn't apply to your device, do not leave it blank. Include the section and a brief statement explaining why it's not applicable. A submission with missing sections, even ones that genuinely don't apply, looks incomplete to a reviewer and will get kicked back.
Section 6.0: Truthful and Accuracy Statement
The Truthful and Accuracy Statement certifies that all information in the submission is truthful, accurate, and complete. The FDA has provided the exact content of the statement, so there's nothing to write from scratch.
Section 7.0: Class III Summary and Certification
If your device is Class II, which covers most 510(k) submissions, this section contains a single sentence: "This device is not a Class III device." If your device type is Class III but does not require a premarket approval application (PMA), you'll need to provide a summary of the types and causes of safety and effectiveness problems along with supporting data.
Section 8.0: Financial Certification or Disclosure Statement
If you did not perform clinical studies, this section is also a single sentence: "No clinical studies were performed to test this device." If you did perform clinical studies, the form breaks into two paths. The Financial Certification applies if the clinical investigators were not paid beyond the costs of conducting the study. The Disclosure Statement applies if additional payment was made, and it must include documentation of how any bias was mitigated.
Section 9.0: Declarations of Conformity and Summary Reports
This is where you document conformance to any applicable consensus standards. If you tested to recognized standards such as IEC 60601-1 for electrical safety, ISO 10993 for biocompatibility, or IEC 62304 for software, this is where you declare it.
Group 4: Comparing your device vs. predicate(s)
Section 10.0 – Executive Summary
Section 11.0 – Device Description
Section 12.0 – Substantial Equivalence Discussion
At this point, you’ve made it halfway through your 510(k) submission. Give yourself a pat on the back and take a few deep breaths. The last half of the 510(k) submission is going to go one of two ways: easy or hard.
If you've kept up with design controls documentation, risk management records, and your quality system throughout development, Groups 4 through 7 are primarily an exercise in organized retrieval. If you haven't, this is where teams spend weeks reconstructing records that should have existed months ago.
Predicate device selection: what's at stake
Before you can write any of the sections in Group 4, you need a solid predicate device, and selecting the right one is more strategic than most first-time submitters realize.
A valid predicate must be a device that FDA has previously cleared or classified, with the same intended use as your device and the same or equivalent technological characteristics. The key decision points are these: the predicate's indications for use set the ceiling for your own indications, the technological characteristics of the predicate determine what comparative testing you'll need to perform, and if your chosen predicate has known safety issues on its record, that history can complicate your review.
Common mistakes in predicate selection include choosing a predicate with more specific indications than your device actually needs (which constrains your cleared use), selecting an older device whose technology is so different from yours that equivalence becomes difficult to establish, and failing to search for multiple possible predicates before committing to one.
Use the FDA's 510(k) database to search cleared devices by product code and review the substantial equivalence discussions in similar cleared submissions. These are publicly available and are one of the most useful resources for understanding what FDA expects to see for devices like yours.
Section 10.0: Executive Summary
The Executive Summary is where you describe your device, compare it to the predicate, and summarize all testing performed. Unlike the 510(k) Summary from Section 5.0, the Executive Summary is not released publicly after clearance. That means you can be more detailed here. A comparison table is the standard approach: put your device and the predicate side by side across indications for use, technological characteristics, and performance. Be specific and thorough. This table sets the stage for the reviewer's entire evaluation.
Section 11.0: Device Description
The Device Description is not the brief marketing description your team uses in pitch decks. This is the technical record of what your device is, built from your design outputs. Pull detailed drawings with dimensions and tolerances for each device, accessory, and component. For any component that comes into patient contact, list the specific materials and include material specifications. Reference any applicable device-specific guidance documents and confirm you've addressed all description requirements within them. The device description section gets the FDA reviewer intimately familiar with your device and sets the stage for Section 12.0.
Section 12.0: Substantial Equivalence Discussion
The basis for the 510(k) submission is to show that your new device is safe and effective, because it’s a lot like another device that’s already been reviewed and cleared by the FDA.
Go step by step through indications for use, technology, and performance, comparing your device to the predicate point by point. The table from Section 10.0 is a useful starting point, but this section should include the narrative rationale, not just the comparison. If your device uses different technology, you need to demonstrate that it is at least as safe and effective as the predicate. If bench and animal testing alone are not sufficient to establish equivalence, clinical data may be required. The more carefully this section is built, the fewer Additional Information requests you'll receive.
Consider a Q-Sub before you finalize
If your submission has any complexity, such as novel technology, a predicate device that isn't a clean match, or performance characteristics that differ from the predicate and require testing justification, a Pre-Submission (Q-Sub) meeting with FDA is worth serious consideration.
A Q-Sub lets you ask FDA specific questions about your submission before you file: which testing is sufficient to establish substantial equivalence, whether your proposed predicate device is appropriate, and what your documentation needs to cover for a specific section. FDA's responses are documented and provide a level of certainty about your submission strategy that is difficult to achieve any other way. A Q-Sub does add time upfront, but for complex submissions it consistently reduces review time overall.
Group 5: Ensuring patient safety
Section 13.0 – Proposed Labeling
Section 14.0 – Sterilization and Shelf Life
Section 15.0 – Biocompatibility
The same principle applies in Group 5 as in Group 4: comprehensive, organized design controls and risk management documentation make this section fast. Missing or incomplete records make it slow and expensive.
Section 13.0: Proposed Labeling
Labeling includes more than your device label. It encompasses your instructions for use (IFU), package insert, and any patient labeling. Pull this from your design outputs. While this should be your final version, expect the possibility of changes during the review and clearance process.
Note that the FDA considers information on your company website about your product as labeling. This means you are not permitted to market your device prior to receiving 510(k) clearance, and your website copy, sales materials, and any public-facing content about the device should not make performance claims until the decision is in hand.
Before you finalize the labeling section, confirm that the indications for use on your IFU match your indications for use statement from Section 4.0. Any discrepancy here is a straightforward rejection reason.
Section 14.0: Sterilization and Shelf Life
The first section on testing is Section 14.0 – Sterilization and Shelf Life.
If your device is non-sterile, state that explicitly. Don't assume the reviewer will infer it from your labeling. For sterile devices, you need to demonstrate both that the device is sterile at the end of its stated shelf life and that it still performs as expected. This typically includes accelerated age testing. If you intend to make a shelf-life claim, performance testing over the stated shelf life is required to support it. If shelf-life testing is not applicable to your device because there is no meaningful risk of time-based performance degradation, include a brief explanation of why.
Section 15.0: Biocompatibility
If your device has any components in direct or indirect patient contact, biocompatibility testing is almost certainly required. Per the Refusal to Accept (RTA) checklist, you need to include both the protocol and the test reports. The only exception is if your device is identical in both material composition and manufacturing process to the predicate device. Since you would need to be the legal manufacturer of the predicate device to know its manufacturing processes with certainty, this exception applies in very few real-world cases.
Group 6: Software and electrically powered components
Section 16.0 – Software
Section 17.0 – Electromagnetic Compatibility and Electrical Safety
If your device has no software or electrical components, skip ahead to Group 7. Before you do, include both sections in your submission with a single sentence stating the section is not applicable. As with every section in this submission, a blank page reads as an incomplete submission.
Section 16.0: Software
Start with the software level of concern, either Minor, Moderate, or Major, and your rationale for that designation. The rest of the section covers requirements, specifications, risks, and verification and validation activities related to the software.
The amount of documentation required scales with your level of concern. A Major level of concern submission includes a full software requirements specification, architecture design chart, software design specification, traceability analysis, hazard analysis, and verification and validation protocols and reports. IEC 62304 is FDA-recognized and provides the most widely used framework for organizing this documentation. If your team has been following IEC 62304 throughout development, this section primarily involves organizing and presenting what you already have.
Section 17.0: Electromagnetic Compatibility and Electrical Safety
Any device with electrically powered components, whether or not those components are in patient contact, needs to demonstrate electromagnetic compatibility (EMC). In plain terms, this means showing that your device does not interfere with other electrical devices and cannot be meaningfully interfered with by them. The recognized standard for this testing is IEC 60601-1-2. If your electrically powered components are in patient contact, you'll also need to demonstrate patient safety per IEC 60601-1, including Amendment 1 and Amendment 2.
Group 7: Performance testing
Section 18.0 – Performance Testing – Bench
Section 19.0 – Performance Testing – Animal
Section 20.0 – Performance Testing – Clinical
You’re in the home stretch when it comes to preparing your 510(k) submission: the performance testing sections.
Groups 1 through 6 set the context and establish the regulatory framing. Group 7 is where you prove the case for substantial equivalence with data.
Every section in Group 7 follows the same structure regardless of the type of testing it covers. Each section needs a protocol, including the objective, sample size, test method, study endpoint, and pass/fail criteria, along with a corresponding report with a clearly stated summary, analysis, and conclusion. Do not embed raw test data in the body of the report. If raw data needs to be included in the submission, put it in an appendix.
Hopefully, you were following the design control requirements laid out in 21 CFR Part 820.30 and compiling these sections is going to be nothing more than printing out your design verification and validation test protocols and reports.
Section 18.0: Performance Testing — Bench
This section will likely contain the bulk of your design verification and validation testing. If you've been documenting your verification and validation activities as they occurred under QMSR, this section is largely a compilation exercise.
Section 19.0: Performance Testing — Animal
Animal testing is not required for most 510(k) submissions. It's required only when bench testing is insufficient to establish substantial equivalence, or when your device uses different technology from the predicate and additional evidence of safety and effectiveness is needed. FDA will always consider scientifically supported alternatives when proposed with adequate rationale.
If you believe animal testing may be required for your submission, engage with the relevant FDA review branch early in your testing planning. A Pre-Submission (Q-Sub) meeting is the most direct way to get FDA's guidance on what's needed before you invest in studies that may not meet the evidentiary standard.
Section 20.0: Performance Testing — Clinical
Clinical testing is also not required for most 510(k) submissions, and FDA will always consider scientifically supported alternatives to clinical studies when proposed with adequate rationale.
If clinical testing is required, your first step is determining whether your study is significant risk or non-significant risk. Significant risk studies must be conducted under Investigational Device Exemption (IDE) regulations per 21 CFR Part 812. Non-significant risk studies follow the abbreviated requirements under 21 CFR Part 812.2(b). Regardless of risk designation, all clinical studies must comply with the regulations governing institutional review boards (21 CFR Part 56) and informed consent (21 CFR Part 50).
The very last thing you should do before you submit your 510(k) is grab the RTA checklist. Go through the RTA checklist and write down the page numbers where everything can be found. If you notice anything is missing, this gives you the chance to add it. It will also make it a little easier for your reviewer.
Common 510(k) rejection reasons and how to avoid them
Getting the sections right matters, but the reasons most submissions get rejected aren't buried in the technical testing. They're in the fundamentals. Here are the causes of RTA decisions and reviewer AI requests that come up most often.
-
Mismatched indications for use. If the indications for use on your cover sheet, your 510(k) Summary, your IFU, and your Substantial Equivalence Discussion don't all match, FDA will ask you to reconcile them. Check all four documents against each other before you file.
-
Missing "not applicable" statements. Any section left blank is a missing section in the reviewer's eyes. Every section that doesn't apply needs a brief written statement explaining why.
-
Incomplete or missing test reports. Referencing testing without including the protocol and the report is not sufficient. FDA wants to see both, with pass/fail criteria clearly stated and results clearly reported.
-
Predicate device mismatch. If the predicate device you've selected has substantially different technological characteristics and you haven't adequately justified equivalence, FDA will either ask for additional testing or ask you to select a different predicate.
-
Labeling inconsistencies. Device label, IFU, and website language that doesn't match the cleared indications for use is a common source of post-submission clarification requests. Align all of it before filing.
-
Outdated or incorrect forms. Using a superseded version of FDA Form 3601 or 3514 will result in an RTA. Always download forms fresh from the FDA website before completing them.
The best insurance against all of these issues is the RTA checklist. Before you submit, go through the checklist in full, confirm each item is present, and note the page number in your submission where it can be found. If anything is missing, the checklist gives you the chance to add it before FDA sees the gap.
What happens after you submit
While you should feel good about getting your 510(k) submitted, you haven't crossed the finish line yet. Now the review process begins. Here's what to expect.
-
Acceptance review. After you file, FDA has 15 days to determine whether your submission meets the threshold for acceptance, meaning it contains all required sections and isn't missing any elements that would prevent a meaningful review. If your submission is refused to accept, FDA will tell you why and give you the opportunity to correct and refile.
-
Substantive review. Once accepted, FDA has 90 days to complete its substantive review. The clock is measured from the date of acceptance, not the date of filing. In practice, the average total review time is longer than 90 days because of AI requests.
-
Additional Information (AI) requests. If FDA needs more information to complete the review, they'll issue an AI request and the 90-day clock pauses. When you respond, the clock restarts. Multiple rounds of AI requests are common for complex submissions and almost always preventable with better upfront preparation. If you receive an AI request, respond to every point specifically. Vague or partial responses typically generate follow-up requests.
-
The decision. FDA will issue one of three decisions: substantial equivalence (clearance), not substantial equivalence (not cleared), or a request for reclassification. If you receive a not-substantial-equivalence determination, you can either refile with a different predicate or seek reclassification through the De Novo pathway if appropriate. Clearance is not the same as FDA approval. Class II devices cleared through the 510(k) pathway are not "FDA approved" devices, and that language should never appear in your labeling or marketing materials.
Preparing 510(k) submissions with a quality system built for the job
Congratulations! You’ve made it through compiling your entire 510(k) submission!
If this process felt more documentation-intensive than you expected, that's the point. The 510(k) is not a one-time administrative exercise. It's a structured account of everything your team did to design, develop, test, and validate a medical device. Teams that treat quality documentation as a continuous practice, building records as they work rather than as they prepare to file, consistently produce cleaner submissions, receive fewer AI requests, and get to clearance faster.
The inverse is also true. The teams that spend the most time in the back half of their 510(k) are almost always the ones who deferred documentation, used disconnected tools, or tried to reconstruct their design controls and risk management records under submission pressure.
If your quality system is making submission prep harder than it should be, get your free demo of Greenlight Guru today and see how the right eQMS can simplify getting to market.
A Step-By-Step Guide to Preparing Your FDA 510(K) Submission